
The Missing Clamp: Inside the Hidden Crisis in Surgical Supply Chains
Inside the operating room supply crisis that delays surgeries, sends nurses running down hallways, and occasionally harms patients, and the Chinese hospitals that may have found a fix.


The patient is already on the table, already anaesthetized, when someone notices the tray is wrong.
It happens in hospitals every day, in operating rooms on every continent. A nurse scans the sterile field. A surgeon reaches for an instrument and it is not there. The procedure is orthopaedic, a knee replacement, and the tray that arrived from the sterile supply department, after a half-hour journey through the hospital, contains instruments for a different operation. Someone has to leave the room. Someone has to make calls. The surgeon waits. The anaesthesiologist watches the clock. The patient, oblivious and vulnerable, continues to breathe through a tube.
In the best case, the right tray arrives within minutes and the procedure carries on. In a less fortunate version, the case is postponed. The patient wakes up to learn their surgery did not happen. And the operating room, one of the most expensive spaces in medicine, costing a U.S. hospital somewhere between $10 and $20 per idle minute, has just burned through another hour for nothing.
These are not rare edge cases. They are systemic. And the supply chain that produces them has been running essentially the same way for decades.
“Nearly 40 percent of OR personnel have personally cancelled a case because supplies were missing. Sixty-nine percent have experienced delays for the same reason.”
A body of research now catalogues the scale of this problem in granular, uncomfortable detail. It draws on studies from the United States, the United Kingdom, France, Canada, and Australia. It describes an operating room logistics system that is, in critical ways, still dependent on human memory, paper counts, and someone physically running down a hallway.
And then it describes what a cohort of hospitals in China has started doing instead, and the numbers are striking enough that hospitals in Europe and North America are beginning to pay attention.
104 Ways a Tray Can Go Wrong
The nerve centre of surgical logistics is a department that most patients have never heard of: the Central Sterile Supply Department, or CSSD. Every reusable surgical instrument in a hospital, the clamps, the retractors, the drill bits, the tiny forceps used in eye surgery, flows through the CSSD. Instruments come in dirty, get cleaned and sterilized, get packed into trays organized by procedure type, and go back out to operating rooms. In most hospitals, this entire process is managed by hand. A study published in BMC Surgery set out to count exactly how many ways that can go wrong.
The researchers followed 6,553 individual instruments through 153 trays at a major academic medical campus. They mapped 104 distinct human tasks in the instrument cycle. When they tallied the error risk across all of them, the number came out to 4.8 errors per instrument. More than 88 percent of those errors came from what the study called failures of visualization, the inspection, identification, and assembly work that humans do under time pressure in a sterile processing environment. When an error was not caught, the average delay it caused was 10 minutes. At a single two-hospital campus, the annual cost of instrument-associated OR delays was estimated at between $6.75 million and $9.4 million.
That’s at one campus. A review of UK incident data identified 161 instrument-related patient safety incidents over five years, including five cases that required reoperation. A prospective study of cardiac surgery equipment found that 80 percent of procedures experienced at least one equipment malfunction. In the most extreme category, retained surgical items, meaning instruments or materials left inside a patient, a multicenter study in the Joint Commission Journal found one large U.S. health system was experiencing a harm event of this kind every eight days.
BY THE NUMBERS: THE COST OF SUPPLY CHAIN FAILURE
$9.4M estimated annual cost of instrument delays at a single two-hospital U.S. campus
80% of OR cases experience at least one surgical equipment malfunction
87% of reusable instruments on a typical tray go unused per case
40% of OR staff have personally cancelled a case because supplies were missing
20% of a clinician’s work week spent on supply-chain management tasks
Part of the problem is the trays themselves. A scoping review in BMC Health Services Research covering 48 studies found that surgical trays have a natural tendency to expand over time. Surgeons request instruments be added to accommodate their preferences; almost no one removes anything. The result is trays that are heavier than they need to be, take longer to sterilize, and present more assembly checkpoints where a mistake can hide.
A Vizient analysis across four surgical services found that 87 percent of reusable instruments on trays went unused in any given case. Neurosurgery trays showed utilization as low as 21.9 percent. For every five instruments loaded, cleaned, sterilized, and transported to the operating room, four never leave the tray.
There is evidence that rationalizing trays helps. A PLOS One study on laparoscopic tray consolidation found that replacing multiple specialty-specific trays with one standardized set cut the total instrument count by 255, saved over $55,000, and improved staff satisfaction from 50 percent to 97 percent. But a commentary in the Journal of Thoracic and Cardiovascular Surgery explains why change is slow: surgical specialties guard their preferences, and hospital budgeting structures do not reward departments that use fewer instruments. The incentives run the wrong way.
The numbers get starker the closer you look. A landmark observational study at a large academic medical center in Chicago published in the Journal of the American College of Surgeons tracked 49 procedures across four surgical services and found instrument use rates of 13 percent in otolaryngology, 15.5 percent in plastic surgery, 18.2 percent in bariatric surgery, and 21.9 percent in neurosurgery. The study also found a direct relationship between tray size and error rate: the more instruments on a tray, the lower the use rate and the higher the chance that something goes wrong during assembly. Every instrument cleaned unnecessarily costs between $0.35 and $0.51 to reprocess -- a small number that compounds into a very large one across hundreds of thousands of cases a year.
A 2025 systematic review published in BJS Open -- covering studies from across Europe and North America -- found that simply removing redundant instruments from trays could reduce costs by between 32 and 78 percent per procedure, depending on the specialty. One study within the review cut a total hip arthroplasty tray by 49 percent and saved 7.16 kilowatt-hours of energy and 1.61 kilograms of waste per case, just from the reduction in sterilization wrapping and processing. The review authors note that the operating room generates 20 to 30 percent of all hospital waste and accounts for 30 to 60 percent of total hospital costs -- making the tray problem not just an efficiency issue but an environmental and financial one at institutional scale.
The sterilization cost alone makes the case. A study on surgical tray optimization in pediatric surgery published in the Journal of Pediatric Surgery at a large academic medical center estimated annual instrument cost savings of between $53,000 and $531,000 across just five surgical sections after tray rationalization, depending on assumed instrument lifespan. Labor savings from reduced count, decontamination, and packing time reached as high as $20,400 per year for a single tray. And an optimized knee replacement tray study found that sealed standardized containers reduced OR and sterile processing turnover time by 57 minutes per case and generated estimated annual savings of $249,245 at a single site -- while also cutting the number of trays required per procedure by an average of three.
What makes the tray problem particularly resistant to change is that it is invisible to almost everyone involved. A survey of OR personnel on cost awareness published in the Journal of the American College of Surgeons found that only 16.4 percent of estimates made by nurses, surgical technicians, anesthesiologists, and surgeons were accurate within 50 percent of the actual price of commonly used items. Staff do not know what instruments cost to reprocess, so they have no way to weigh the cost of opening an oversized tray against the inconvenience of requesting a streamlined one. The waste is structural and largely unobserved -- until someone measures it.
PART TWO
The Nurse Who Had to Leave
Inside the operating room, there is a figure whose role is easy to overlook from the outside but whose presence is considered critical to patient safety: the circulating nurse. Unlike the scrubbed members of the surgical team, the circulating nurse moves freely around the room. She monitors the entire operative field, keeps track of instruments and supplies, coordinates communication between the team and the outside world, and serves as what patient safety literature calls the patient’s primary advocate while the patient is incapable of advocating for themselves.
When a supply is missing, the circulating nurse is usually the person who has to go get it. AORN -- the Association of periOperative Registered Nurses, which sets professional standards for OR nursing in the United States, has issued guidance explicitly warning against nurses leaving the operating room during intubation or extubation -- the most dangerous phases of general anaesthesia. Leaving to retrieve a forgotten supply item during those moments is a patient safety violation. If an airway emergency occurs while the nurse is down the hall fetching a clamp, the room has lost its most mobile safety officer.
The data suggest these trips are not occasional aberrations. A scientific statement on cardiac OR human factors published in Circulation found that when surgical teams held proper preoperative briefings -- getting supply needs on the table before the patient was anaesthetized -- nurses made fewer mid-procedure trips for missing supplies. The implication is that without those briefings, those trips are routine. A French prospective study on OR supply waste measured circulating nurses spending as much as 26.3 percent of operative time outside the operating room, mostly responding to supply requests that arose after the procedure had started.
“The circulating nurse is the patient’s primary advocate while the patient is incapable of advocating for themselves. When the supply chain fails, she leaves the room.”
A 2025 narrative review of operating theatre safety found that distractions and interruptions in the operating theatre occur as frequently as 11 to 12 times per hour. Supply-chasing trips are one thread in that larger fabric of disruption -- but they are one of the few that take the safety monitor entirely out of the room.
PART THREE
What’s Happening in the Back Room
Behind every operating room is a satellite supply store, and behind that is a central supply department. In most hospitals, both run on a model that would be recognisable to anyone who has managed a stockroom: people count things by hand, record what they find, order what appears to be running low, and stack new shipments on shelves. A qualitative study of hospital operational failures describes the structural problem this creates. Supply departments replenish on schedules and routines. Clinical units need specific supplies for specific patients at specific moments. Those two rhythms do not match, and the gap generates a constant stream of workarounds that clinical staff absorb mostly invisibly -- until it becomes visible in the form of a cancelled procedure or a nurse leaving the room.
The consequences range from frustrating to dangerous. A Supply Chain Dive investigation into hospital inventory automation described a hospital losing up to $15,000 a month to expired inventory before automation -- products sitting on shelves past their use-by date because no one had real-time visibility into what was there. A Cardinal Health survey of OR personnel found that 24 percent of healthcare providers had seen or heard of an expired product being used on a patient. Twenty-three percent had seen or heard of a patient harmed because supplies were unavailable.
The time burden is just as real. An industry survey reported in Becker’s Hospital Review found that clinicians spend nearly 20 percent of their work week on supply chain tasks -- counting, ordering, chasing, documenting. More than half described inventory management as either complicated or a necessary evil. Most said they wanted to be freed from it.
The inventory count sits at the centre of all of this. Most hospitals still conduct physical inventory counts -- people walking shelves with clipboards or scanners, recording what they see. The counts are periodic, meaning they happen on a schedule rather than in real time.
An HPN Online analysis of hospital supply chain risk found that 78 percent of providers still manually count inventory in at least some departments, with counts consuming one to two staff members for up to two full days per month in a single department. One OR was losing $80,000 a year in expired product waste despite running these counts regularly. A Health Care Management Science study at a 580-bed Alabama hospital found that inventory inaccuracy was failing to account for nearly half a million dollars of consumed medical supplies annually -- generating overstock and shortages simultaneously. Vizient’s analysis of periodic versus perpetual inventory makes the underlying problem plain: in a periodic system, a shortage only becomes visible at the next scheduled count. By then, it may have already disrupted care.
PART FOUR
The Call That Changes Everything
For patients, the most devastating consequence of a supply chain failure is often a phone call the night before surgery, or a conversation in a pre-op bay, telling them the procedure will not be happening today.
A systematic review and meta-analysis in the International Journal for Quality in Health Care found that hospital-system causes accounted for 44 percent of all surgical cancellations -- a larger share than either patient factors or incomplete clinical work-ups. Equipment and supply unavailability was among the dominant contributors. A retrospective cohort study of nearly 30,000 elective surgical cases estimated the direct cost of a cancelled operation at between $5,000 and $8,000, with every unused OR minute costing a U.S. hospital between $10 and $20.
The Cardinal Health survey found that 40 percent of OR personnel had personally cancelled a case because supplies were missing, and 69 percent had delayed one for the same reason. Researchers studying the Canadian cancellation experience have documented the financial and emotional toll on patients who arranged childcare, took time off work, fasted, and mentally prepared -- only to be told it is not happening.
Perhaps the most striking finding: a PMC review of evidence-based approaches to reducing cancellations found that organisationally-driven cancellations had increased 2.5-fold over a five-year period at one institution. The authors called it an institutional calamity. It had been invisible until someone started measuring it.
“Organisationally-driven cancellations increased 2.5-fold over five years at one institution. It had been invisible until someone started measuring it.”
PART FIVE
The Hoarders
When supply systems are unreliable, people adapt. One adaptation is hoarding -- clinical staff stockpiling materials in drawers, under counters, or in personal storage areas as a buffer against the next shortage. It is entirely rational behaviour at the individual level. At the system level, it is expensive. A Cardinal Health survey found that 64 percent of OR personnel admitted to it.
The same logic applies to staffing. When instrument delivery is unpredictable, OR managers schedule extra nurses as a precaution. When sterile processing has high turnover -- driven partly by the physical demands of moving heavy instrument trays -- departments fill the gaps with agency staff at premium rates. The workforce inflates not to deliver better care, but to absorb the variance of a poorly designed logistics system.
A PMC study of hospital operational failures found that nurses spend at least 10 percent of their time working around supply chain problems. A PMC study of perioperative nursing safety notes that carrying heavy instrument trays is classified by AORN as one of seven high-risk ergonomic tasks in the OR environment -- a contributor to the injury rates that drive turnover in sterile processing departments worldwide.
PART SIX
The Library That Became a Hospital
China’s Grade 3A hospitals -- the country’s highest designation, reserved for major regional medical centres -- face a version of this problem at unusual scale. China’s population is ageing rapidly. Demand for orthopaedic and ophthalmic surgery is rising sharply. And the labour model that underlies conventional hospital logistics is under strain.
The response that has emerged in hospitals in Shenzhen, Shanghai, and Guangzhou borrows its logic from an unlikely source: the automated retrieval systems that now run China’s modern public libraries.
In a robotic library -- and China has built hundreds of them -- books are not on open shelves. They are stored in high-density robotic towers. Each book has a machine-readable tag and a precise address in the system. When a reader requests a title, a robotic arm retrieves it and delivers it to a pickup window within minutes. No human enters the stacks. No one misfiles anything. No book goes missing because someone put it back in the wrong place.
The structural parallel with a sterile supply department is close enough to be operational. Sterile instrument trays are discrete objects with unique identifiers, defined storage requirements, and predictable patterns of demand. The critical technical barrier -- that instrument identifiers needed to survive the autoclave -- has been solved.
RFID World China documents tags specifically designed for multi-label surgical tray identification through repeated autoclave cycles -- chips that identify a full tray’s contents in a single batch scan. OFweek Sensors, one of China’s major industrial technology platforms, reports on RFID-enabled sterilization management systems that capture full tray inventories within seconds and automatically update status records through every stage -- washing, sterilization, repair, and dispatch. No manual logging, no clipboards, no periodic counts.
The physical work of moving instruments is handled by autonomous guided vehicles -- robots that navigate hospital corridors, call elevators, and transport sealed instrument bins between the operating suite and the CSSD. Jiankang Jie, China’s leading healthcare industry platform, reports that a typical Grade 3A hospital with 20 operating rooms conducts at least 80 pre-surgical sterile supply deliveries and more than 120 total logistics movements every day. Fulfilling that manually requires three to five dedicated logistics staff per shift. The AGVs run continuously, without shift breaks or competing demands.
The China Mobile Robot Industry Alliance profiles eight major companies competing in the hospital logistics robot market. During the COVID-19 pandemic, these systems were deployed under pressure at Guangdong Provincial People’s Hospital and Wuhan University Zhongnan Hospital -- a real-world stress test under exactly the conditions where manual systems tend to break down. A market overview from Sohu Health describes a logistics ecosystem that now spans box conveyor systems, pneumatic tube networks, AGV fleets, and early-stage drone delivery experiments.
For consumables -- the gloves, sutures, and disposables that OR staff reach for constantly -- Jiankang Jie reports on smart storage rooms now deployed in leading Chinese hospitals: AI-camera-enabled cabinets that track every withdrawal, flag every low-stock item, connect usage directly to patient billing, and generate analytics on exactly what each department is consuming in real time. No one counts, no one stocks, the system does it.
HOW IT WORKS
From Dirty Tray to Sterile Core in Under Ten Minutes
The workflow begins the moment a surgery ends. Used instrument trays are placed into sealed, RFID-tagged transport bins at docking stations in the OR corridor. An AGV arrives -- summoned automatically -- and carries the bin through service corridors to the CSSD. No porter required.
At intake, a fixed RFID reader logs the arrival and immediately triggers a reservation: a clean replacement set is earmarked for the next procedure. The dirty instruments pass through conveyor-fed washer-disinfectors with minimal human handling. After sterilization, a robotic arm places each validated tray into its slot in the automated storage tower.
When a knee replacement is scheduled for 8:00 a.m., the system checks automatically: is the required tray present, sterilized, and within its validity window? If not, an alert goes out with enough lead time to resolve it -- not when the patient is already sedated. If everything is in order, the AGV delivers the tray to the OR sterile core before the surgical team arrives. A second RFID scan confirms: right tray, right patient, right procedure. If there is a mismatch, the bin locks and an alert fires. No one discovers the error by looking at instruments on the table.
WHAT THE NUMBERS SHOW
Reported outcomes from pilot programmes in Guangdong and Zhejiang provinces
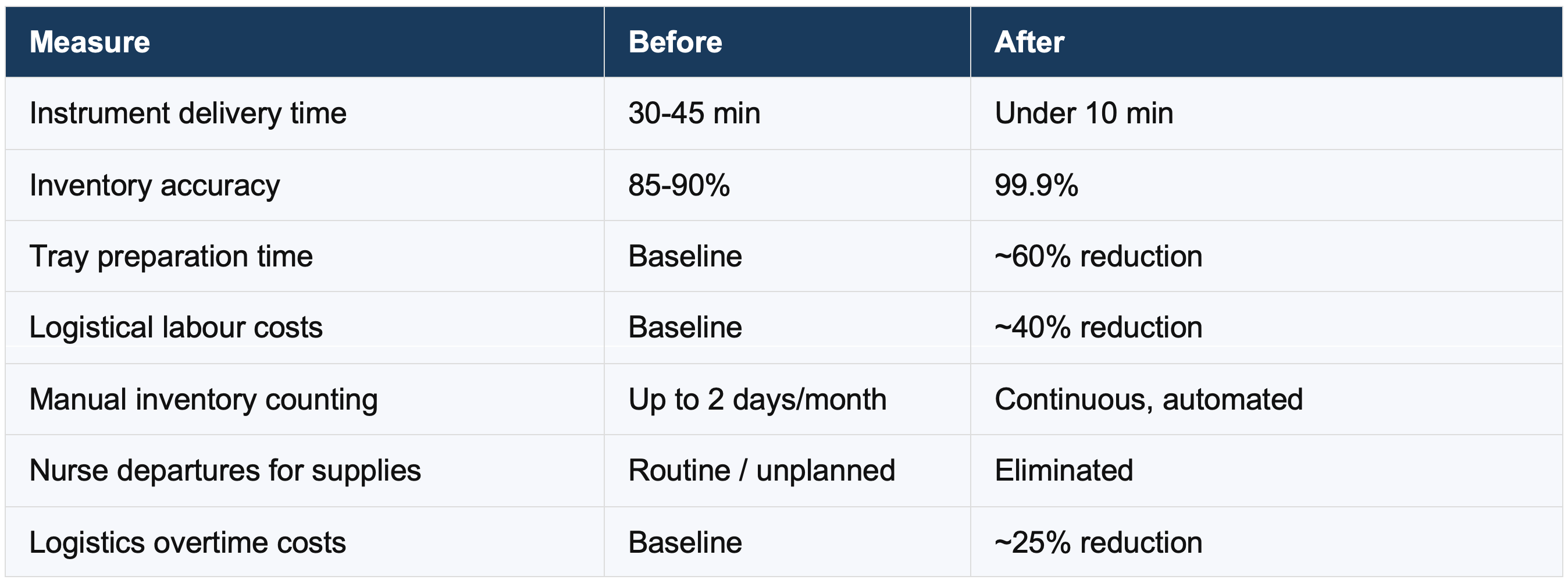
Source: Pilot programme data from Guangdong and Zhejiang provinces; Chinese vendor outcome reports.
The results from early deployments are notable. Pilot data from Guangdong Province reported a 40 percent reduction in logistical labour costs. A three-hospital cohort study in Zhejiang Province found a 25 percent reduction in logistics-related overtime. Elite Robots, one AGV manufacturer, reports a 70 percent reduction in logistics error rates and a 30 percent reduction in staffing costs at implementing facilities.
THE LIMITS
What This Model Cannot Do -- Yet
None of this should be mistaken for a solved problem. Implementation is expensive -- tens of millions of dollars at scale, putting it out of reach for most hospitals. The instrument trays themselves must be standardized to fit the robotic handling system, which means hospitals with years of accumulated non-standard inventory face a significant retrofit before the robots can begin. Any system built on software and robotics also needs a serious manual fallback plan. A network failure or mechanical breakdown can potentially halt instrument delivery across an entire facility.
The evidence base, while encouraging, has gaps. Most outcome data comes from large, well-funded facilities -- exactly the hospitals that were already performing relatively well. And the clinical endpoint that matters most -- whether automated CSSD logistics actually reduces surgical site infection rates -- has not yet been established through long-term prospective study. The mechanism is plausible. The data are not there yet.
CONCLUSION
The Tray Was Always a Data Problem
It is worth stepping back to consider what the conventional surgical supply chain actually is: a set of promises that instruments will be in the right place at the right time, managed largely by human memory, periodic headcounts, and the willingness of clinical staff to run down hallways and improvise when something goes wrong.
For decades, hospitals have treated this as an unavoidable feature of complex healthcare delivery. The Chinese hospitals now deploying robotic CSSD systems are testing a different premise: that it is not unavoidable at all. That the missing clamp, the delayed tray, the nurse who had to leave the room -- these are logistics failures, and logistics problems have engineering solutions.
China’s answer is a robot. It retrieves the tray, verifies the contents, delivers it before it is needed, and never forgets where anything is. Whether that model scales beyond the wealthiest hospitals in the world’s most ambitious healthcare market remains an open question. But for the patient already on the table, waiting for an instrument that should already be there, it represents something the current system mostly cannot offer: a guarantee.
SOURCES AND FURTHER READING
This article draws on a peer-reviewed research review of surgical instrument supply chain failures and automated CSSD logistics. Key studies and sources:
-- BMC Surgery -- instrument error study (6,553 instruments, 153 trays)
-- PMC -- UK instrument-related patient safety incidents
-- Joint Commission Journal -- retained surgical items multicenter study
-- BMC Health Services Research -- surgical tray standardisation scoping review
-- PLOS One -- laparoscopic tray rationalisation study
-- International Journal for Quality in Health Care -- surgical cancellations meta-analysis
-- Health Care Management Science -- inventory inaccuracy at 580-bed hospital
-- Circulation -- cardiac OR human factors scientific statement
-- AORN -- circulating nurse safety guidance
-- OFweek Sensors (Chinese) -- RFID sterilisation management systems
-- Jiankang Jie (Chinese) -- hospital AGV logistics and smart storage
-- China Mobile Robot Industry Alliance (Chinese)
-- RFID World China (Chinese) -- surgical instrument RFID tags
-- Journal of the American College of Surgeons -- instrument use rates by specialty (13-21.9%)
-- BJS Open 2025 -- systematic review of tray optimisation (32-78% cost reduction per procedure)
-- Journal of Pediatric Surgery -- tray optimisation cost savings ($53K-$531K annually)
-- Journal of the American College of Surgeons -- OR staff cost awareness survey (16.4% accuracy)
-- -- --